5212 Claremont Avenue
Oakland, CA 94618• Mon. • Wed. • Fri. • 10am-6:30pm (by appt.) •
• Tues. 12pm-8pm & Thurs. 9am-4pm (by appt.) •Hip Pain
What is “hip pain”? Good question!
We have a language problem here, in that; we use the word “hip” both literally and euphemistically. What I mean is: there is a “Hip Joint”, a “Hip Bone” and a ‘Hip Area” or “Region”.
The Hip Joint is the femoral head and socket joint. The socket is in the “Hip Bone”. See illustration.
The outside of this area, the Hip Region, the “buttocks”, the “Glutes” is where a lot of people have pain.
This pain might not be caused by the hip socket joint. The hip socket joint is where “hip replacement” surgery takes place. Two different people may seem to have the same symptoms, yet one will need and greatly benefit from hip replacement surgery and the other will not. How can you tell?
I’ll tell a story.
E, a 62 year old woman, came into my office in July 2004. She had a hip replacement surgery scheduled for July 13th, the following Tuesday. She had brought her x-rays from her Orthopedist with her. I took a look at the films. The hip socket joints looked normal and symmetrical; in other words, they looked the same — visually, I couldn’t tell which was to be replaced, although she had told me it was to be the right side.
I covered the marker that indicated that one side was the right side. I then had the patient come back to view the films. I asked her what was different about the two hip joints. One should look different from the other if one is to be replaced. She studied them for a moment and concluded they looked the same. I then showed her a textbook picture of a normal x-ray for that region of the body, she concluded that they all looked the same.
On examination it was apparent she had an altered gait and posture and was in obvious pain.
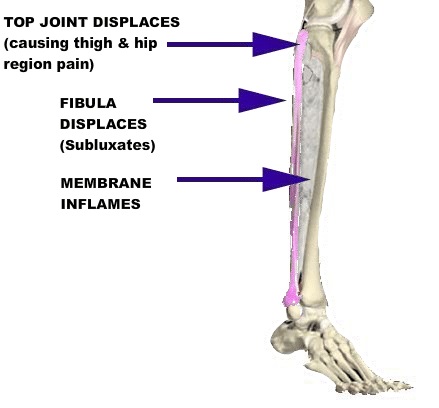
The whole outside of her right leg was painful to the touch and quite hard at rest. The top joint of the fibula and tibia, just below the knee was the worst. When I compressed the fibula to the tibia and maintained 20-30 seconds of pressure, the muscles started to soften. I could touch the outside of the hip area without her flinching, as long as I maintained the compression of the fibula to the tibia. The muscles of this area attach to the upper part of the leg and hip and the lower parts of the leg as well. See Figure 2.
We did a chiropractic adjustment of the fibula and put a strap on it to stabilize the joint.
Her posture and gait changed immediately with the use of the strap. On Friday she was 60-70% improved, said she had canceled her surgery. She missed her Monday appointment because her tile setter didn’t show up at her house and she spent the day laying marble tile on the floor of her entryway! Of course we had a little set-back. (Should I mention she is an attorney? We have an ongoing debate about whether or not law school causes brain damage or it is required as a prerequisite!)
So, in just a couple of treatments, we had decreased her pain and improved her functional capacity to the point that she was hurting herself again! A mark of a successful treatment, I guess. She had to wear the strap regularly for 18 months before the tibia/fibula area became stable.
I do think that she would have been harmed by the surgery. She would have had a terrible wound — the surgery — plus her original, untreated, injury that was the source of her pain and limitations. Frankly, in my opinion, she would have been worse off.
If you’re considering surgery, get evaluated by someone who is not a surgeon, who can look for other causes of your symptoms.