5212 Claremont Avenue
Oakland, CA 94618• Mon. • Wed. • Fri. • 10am-6:30pm (by appt.) •
• Tues. 12pm-8pm & Thurs. 9am-4pm (by appt.) •Wrist + Hand
Wrist pain is a common and costly occupational problem affecting thousands of people every year.
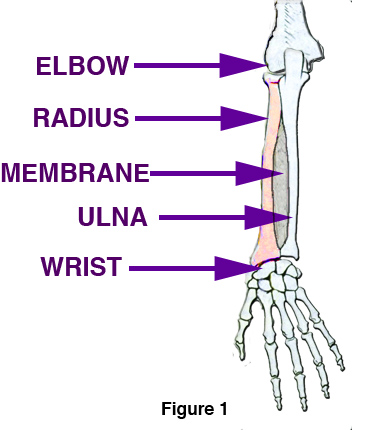 Repetitive stress injuries (RSI) to the hand and wrist have six common forms, with carpal tunnel syndrome (CTS) being the most prevalent. The wrist is comprised of two forearm bones, the ulna and the radius, and in the space at the end of them, eight wrist bones. (See illustration)
Repetitive stress injuries (RSI) to the hand and wrist have six common forms, with carpal tunnel syndrome (CTS) being the most prevalent. The wrist is comprised of two forearm bones, the ulna and the radius, and in the space at the end of them, eight wrist bones. (See illustration)
The common feature of many RSI’s or wrist complaints is loss of joint space — a narrowing and compression of the wrist compartment. What could cause the normal relations of the bones, tendons and nerves to alter sufficiently to result in this painful compression of wrist space?
A common feature of patients complaining of wrist pain is additional pain and tenderness in the forearm and elbow.
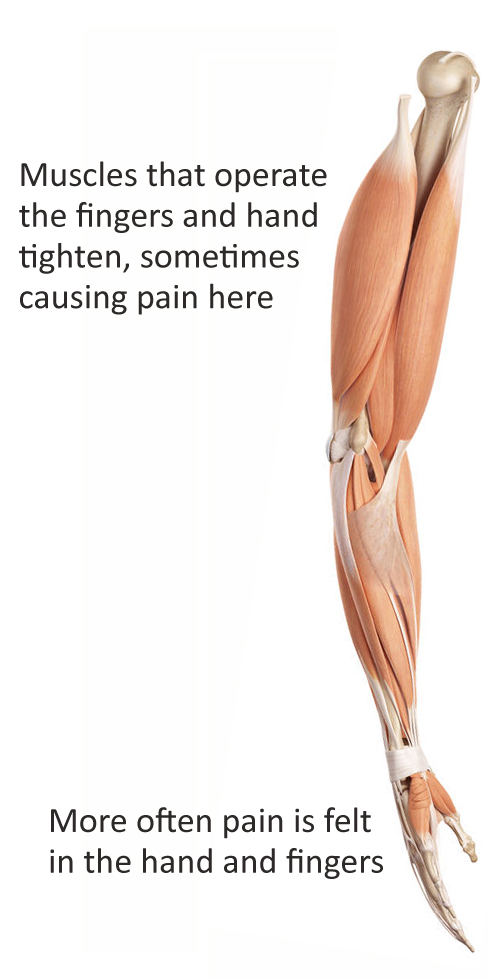
 The muscles that move the fingers and hand start above the elbow (see illustration). Misalignment of the elbow joints results in a defensive tightening of the muscles that operate the wrist and hand, which then causes distress and pain. Activity, especially repetitive movement, makes the distress worse. This indicates that thickening and shortening of these tissues could be part of the syndrome.
The muscles that move the fingers and hand start above the elbow (see illustration). Misalignment of the elbow joints results in a defensive tightening of the muscles that operate the wrist and hand, which then causes distress and pain. Activity, especially repetitive movement, makes the distress worse. This indicates that thickening and shortening of these tissues could be part of the syndrome.
It has been shown that these tendons increase in mass with exercise, i.e. stress. Certainly this condition could cause carpal collapse and loss of joint space in the hand and fingers as well. Also thickening of the tendons through the wrist region causing stenosis could be a consequence of contraction of the flexor-extensor groups.
Deformations of tendons and ligaments have two main components: time and weight.
Persistent passive stretch to reform ligaments and rehydrate discs is used in spinal rehabilitation. Can a similar approach be used on the forearm and muscular and tendonous structures of the hand and fingers? Studies done on intervertebral discs and spinal ligaments indicate that, to overcome the natural elastic deformation of these tissues, a constant stretching force for 12 -15 minutes must be achieved. Increase in length of these tissues occurs only after the natural flexibility of the tissues has been reached. The steepest part of the change curve (length graphed against time) is 20 to 25 minutes after the beginning the session, and there is little change after that.